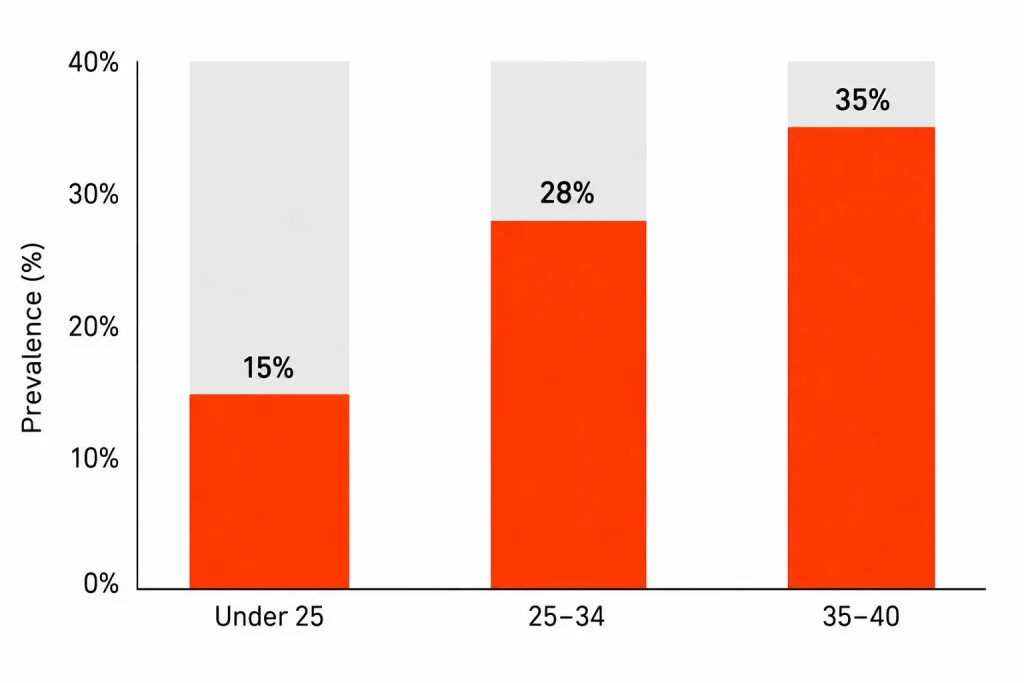
Erectile dysfunction in young men is far more common than most people admit, and the causes are not what mainstream advice usually suggests. ED is not just an old man’s problem. Research now shows that up to 35% of men under 40 experience some degree of erectile dysfunction, and the trend is rising sharply in India and globally.
Most young men who search this topic are hoping to hear it is just stress. Sometimes it is. But often the real picture involves a mix of psychological, hormonal, and lifestyle factors that take more than reassurance to fix.
Indian men face a specific version of this problem: sedentary work culture, poor sleep, high psychological pressure, and a deep reluctance to discuss sexual health openly. That combination is creating a silent epidemic in men who are otherwise considered “fit and healthy.”
What follows is a clear, honest breakdown of every major cause, how to identify which one applies to you, and what to actually do about it.
The Short Answer
- Performance anxiety and psychological stress are the most common causes of erectile dysfunction in young men, creating a vicious cycle where fear of failure triggers actual failure.
- Pornography use has been linked to ED in young men through altered arousal patterns, though the evidence is still debated and individual effects vary.
- Hormonal imbalances, especially low testosterone, are increasingly being found in young Indian men due to poor sleep, obesity, and chronic stress.
- Lifestyle factors including smoking, excessive alcohol, poor diet, physical inactivity, and recreational drug use all directly impair the blood flow and nerve function needed for erections.
- Organic causes such as endothelial dysfunction, diabetes, and cardiovascular risk factors are no longer rare in men under 30, especially those with sedentary lifestyles and poor metabolic health.
Why Is ED in Young Men Becoming More Common?
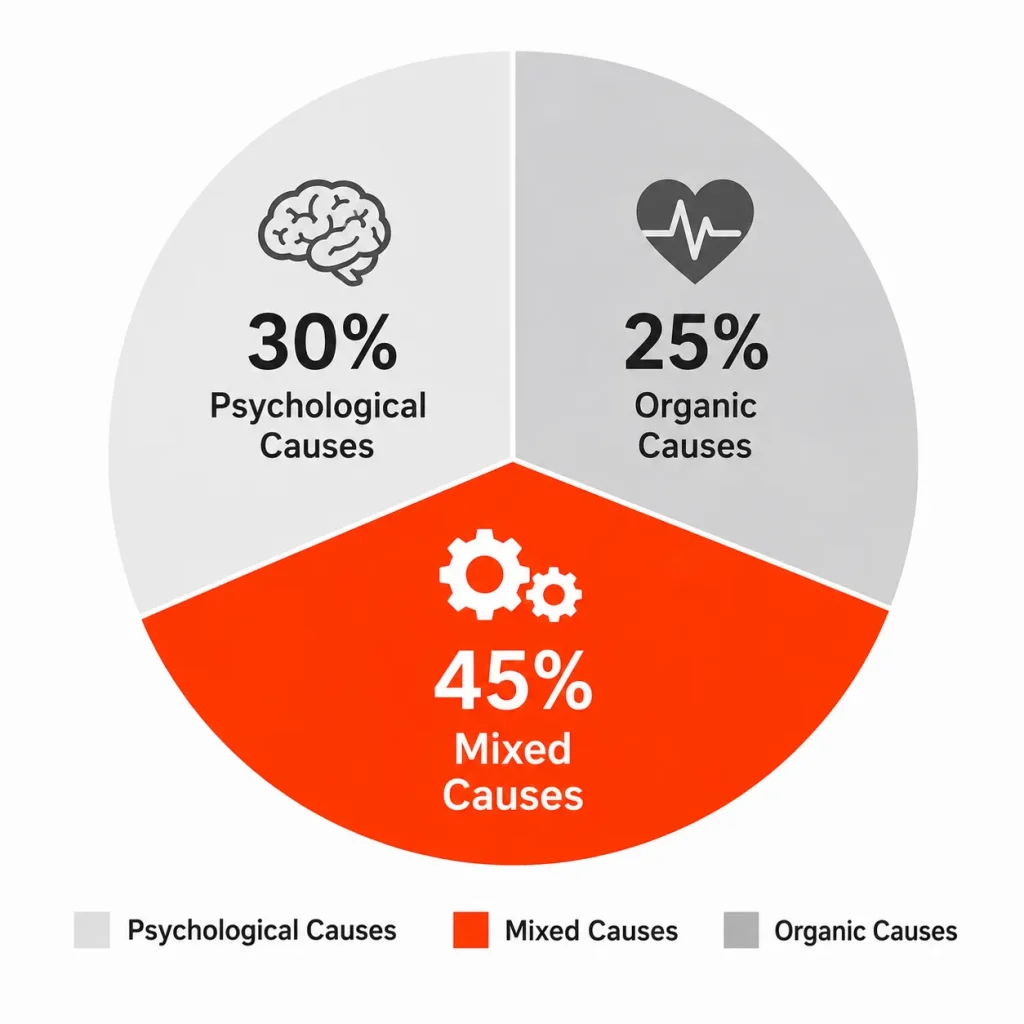
Erectile dysfunction was once considered almost exclusively a disease of older men. That assumption is now outdated. A 2025 narrative review published in PMC/NIH analysed nearly 2,000 studies on ED in men under 40 and found prevalence rates as high as 35%, with both psychogenic and organic causes increasingly present in younger populations.
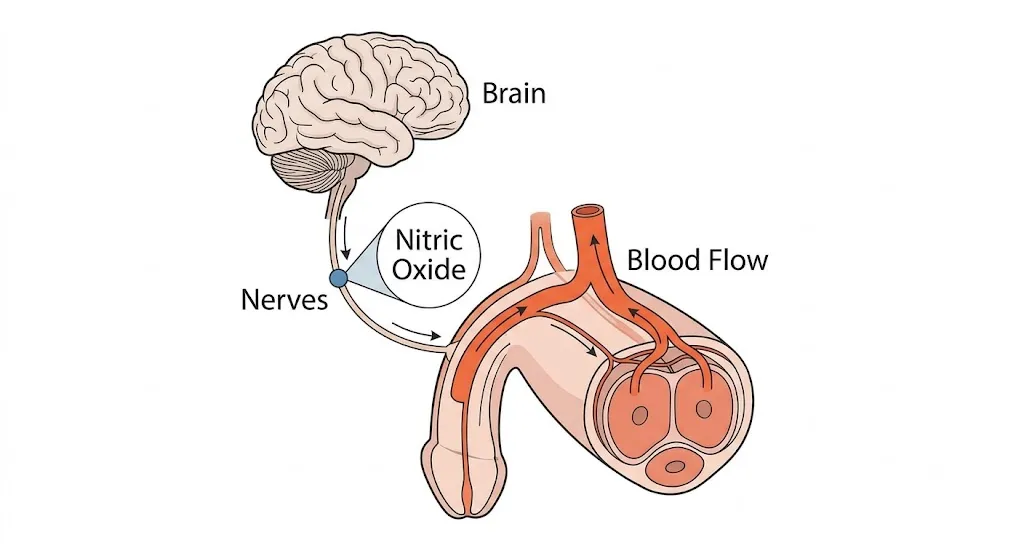
The mechanics of an erection are deceptively complex. It requires a coordinated sequence: sexual arousal signals from the brain, nervous system activation, release of nitric oxide in penile blood vessels, smooth muscle relaxation, and a sustained increase in blood flow. Any disruption in that chain, whether from anxiety, hormonal deficiency, poor vascular health, or nerve damage, can break the process.
For Indian men specifically, the risk landscape has shifted considerably. Desk jobs, late nights, heavy reliance on ultra-processed foods, and the psychological weight of career and family expectations create conditions where ED can develop even in men in their early 20s. Data from the Institute of Andrology and Sexual Health India found that roughly 25 out of every 100 ED patients in India are now under 30, a number that was just 5 to 7 a decade ago.
The low testosterone in young men connection matters here too. Low testosterone does not just reduce libido. It affects mood, vascular function, and the neurological signals that initiate arousal, all of which feed directly into ED risk.
The Major Causes: A Full Breakdown
Performance Anxiety: The Most Common Cause in Young Men
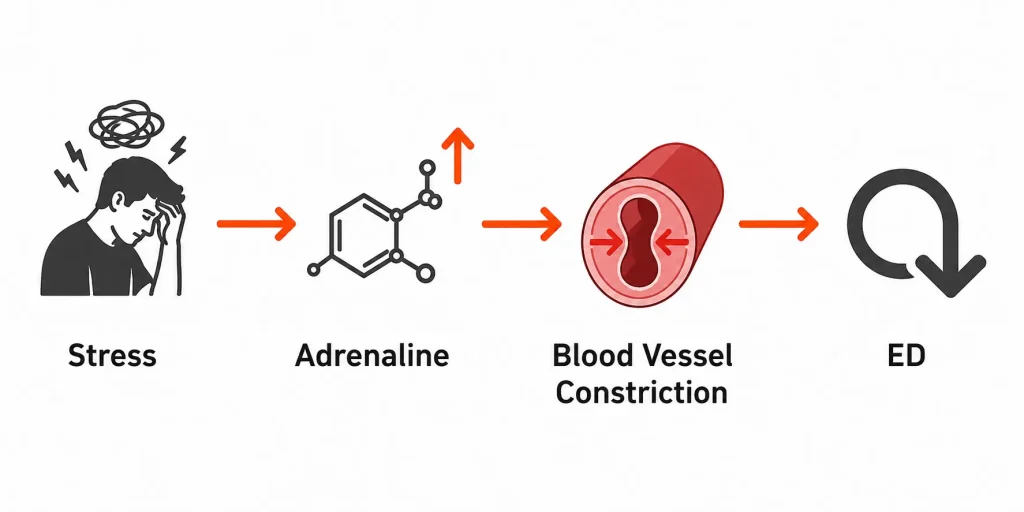
Performance anxiety is the single most frequently identified cause of ED in otherwise healthy young men. It works through a mechanism that is almost cruel in its circularity: the fear of not getting an erection triggers the exact physiological response that prevents one.
When the brain perceives threat, the sympathetic nervous system activates the fight-or-flight response. This floods the body with adrenaline and noradrenaline, which constrict blood vessels throughout the body, including in the penis. Erections require blood vessel dilation, not constriction. Anxiety directly blocks that.
A review published in Translational Andrology and Urology via PMC noted that young men with ED are frequently dismissed with reassurance and no further investigation, which worsens outcomes. One failed erection becomes two, and soon the anticipation of failure is enough to guarantee it.
In the Indian context, this is compounded by the cultural taboo around discussing sexual difficulty. Men who cannot talk about the problem cannot address the anxiety around it, so the cycle deepens in silence.
Verdict: If you maintain normal erections during sleep or self-stimulation but struggle with a partner, psychological cause is very likely the primary driver.
Psychological Stress and Depression
Chronic stress and depression interfere with erectile function through multiple overlapping pathways. Cortisol, the primary stress hormone, suppresses testosterone production at the level of the hypothalamus. Sustained high cortisol levels impair the hormonal signals that support sexual arousal and erection.
Depression reduces dopamine activity in the brain’s reward system, which directly lowers libido and reduces the arousal response. Research found a significant association between ED and symptoms of depression and anxiety in men aged 18 to 40, with the relationship described as bidirectional: depression contributes to ED, and ED worsens depression.
For men dealing with academic pressure, job instability, financial stress, or relationship conflict, the psychological burden alone can produce ED without any physical cause at all. And in India, where mental health still carries heavy stigma, these issues frequently go unaddressed for years.
If your lifestyle includes chronic sleep deprivation or unmanaged stress, our article on exercises for heart health that improve cardio naturally covers physical strategies that directly reduce cortisol and improve vascular function, both of which matter for ED.
Verdict: If ED arrived alongside a period of high stress, low mood, or poor sleep, the psychological-hormonal axis is almost certainly involved.
Low Testosterone and Hormonal Imbalances
Testosterone plays a direct role in sexual desire, arousal signal strength, and the health of penile tissue. Low testosterone, also called hypogonadism, is no longer rare in young men. The trend toward low-T in men in their 20s and 30s is well documented, and the causes are largely lifestyle-driven.
Obesity increases the conversion of testosterone to estrogen via an enzyme called aromatase, which is found in fat tissue. Poor sleep, particularly less than 6 hours per night, can reduce testosterone levels significantly since most testosterone is produced during deep sleep. Chronic stress, as noted above, suppresses the entire hormonal signalling chain.

Thyroid dysfunction and elevated prolactin levels are other hormonal causes that are frequently missed in young men presenting with ED. Without basic blood work, these remain invisible.
For Indian readers specifically, magnesium and zinc deficiency are relevant here. Both minerals are involved in testosterone production, and Indian diets, particularly vegetarian ones, are often low in bioavailable zinc. Deficiency in these minerals compounds the hormonal side of ED risk.
Verdict: Low testosterone as a cause requires a blood test to confirm. If libido is also reduced (not just erection quality), hormonal investigation is worthwhile.
Pornography Use and Altered Arousal
This is the most debated cause on this list, and the honest answer is that the evidence is real but not fully settled. A 2021 study in the Journal of Medical Internet Research (PMC) surveyed over 3,400 men aged 18 to 35 and found associations between problematic pornography consumption and erectile dysfunction, though causality was not fully established.
The proposed mechanism involves sensitisation of the brain’s reward system. Frequent exposure to high-stimulation pornography may gradually require greater novelty or intensity for the same level of arousal, making the less-stimulating reality of partnered sex feel less engaging by comparison. This is not a moral argument; it is a neuroscience one, and the dopamine reward pathways involved are well understood.
The clearest clinical signal is situational ED: erections work normally during masturbation with pornography but fail or are reduced with a partner. If this pattern applies, pornography use is worth examining as a contributing factor.
No formal diagnosis for “porn-induced ED” exists in DSM-5 or ICD-11. This is not the same as saying the phenomenon does not exist. It means it has not been formally codified yet. The evidence for psychological alteration of arousal patterns is genuinely there.
Verdict: Not everyone who uses pornography will develop ED. But if the situational pattern is present, reducing use is a low-risk intervention worth trying.
Lifestyle Factors: Smoking, Alcohol, Drugs, and Physical Inactivity
These causes are often listed but rarely explained mechanically. Here is what actually happens:
Smoking damages the endothelium, the thin inner lining of blood vessels. The endothelium produces nitric oxide, which is the primary chemical signal that causes penile blood vessels to dilate during arousal. Smoking-related endothelial dysfunction directly impairs erection quality, often years before other cardiovascular symptoms appear.
Alcohol suppresses the central nervous system, reducing the sensitivity of arousal signals. Chronic alcohol use also damages liver function, which affects hormone metabolism and testosterone clearance.
Recreational drugs including cannabis, cocaine, and anabolic steroids all carry direct ED risk. Anabolic steroids suppress the body’s natural testosterone production through negative feedback on the hypothalamic-pituitary axis, often causing ED even while testosterone levels appear artificially elevated.
Physical inactivity reduces cardiovascular efficiency and contributes to the metabolic risk factors, including elevated blood pressure, insulin resistance, and abdominal obesity, that directly impair penile blood flow.
Organic Causes: Vascular and Metabolic Disease in Young Men
This category surprises most people. Subclinical cardiovascular disease, which means endothelial dysfunction and early arterial stiffness without overt symptoms, is increasingly identified in young men who present with ED. A study of men under 40 with ED found they had significantly higher blood pressure, cholesterol, and inflammatory markers compared to age-matched controls, pointing to early vascular disease as an underlying driver.
Type 2 diabetes, once rare in young adults in India, is now prevalent in urban populations due to sedentary lifestyle and high carbohydrate diets. Poorly controlled blood sugar damages both nerve fibres and small blood vessels, both of which are required for normal erectile function.
The Delhi AQI and sperm health connection is worth noting here too. Long-term air pollution exposure is associated with systemic endothelial inflammation, which overlaps directly with vascular ED risk.
Verdict: If you are young, overweight, sedentary, or have a family history of diabetes or cardiovascular disease, organic causes deserve proper investigation, not dismissal.
Causes of ED in Young Men: At a Glance

| Cause | Primary Mechanism | Key Signal | How Common in Young Men | Action |
|---|---|---|---|---|
| Performance anxiety | Sympathetic nervous system activation, blood vessel constriction | ED with partner, normal with self-stimulation | Most common cause | Psychological intervention, CBT |
| Depression and chronic stress | Cortisol suppression of testosterone, reduced dopamine | ED alongside mood changes, poor sleep | Very common | Mental health support, lifestyle change |
| Low testosterone | Reduced arousal signalling, poor vascular tone | Low libido alongside ED | Increasingly common | Blood test, lifestyle, medical review |
| Pornography-related | Altered dopamine reward sensitivity | Situational: works with porn, not with partner | Debated, rising | Reduce use, rebalance arousal |
| Smoking | Endothelial damage, reduced nitric oxide | Gradual worsening, often symptom-free otherwise | Moderate | Quit smoking |
| Alcohol and drugs | CNS suppression, hormonal disruption | Worse with use | Moderate | Reduce or eliminate |
| Metabolic and vascular disease | Impaired blood flow, nerve damage | ED alongside weight gain, fatigue, frequent urination | Rising in India | Medical investigation |
How the Body Produces an Erection (And Where It Goes Wrong)
An erection begins in the brain, not the penis. Sexual arousal triggers nerve signals that travel down the spinal cord and into the pudendal nerve network in the pelvis. These signals cause the smooth muscle in the corpora cavernosa, the two cylindrical chambers of erectile tissue in the penis, to relax.
When smooth muscle relaxes, blood flows rapidly into those chambers, creating hydraulic pressure that produces the erection. The blood stays in because the increased pressure compresses the veins that normally drain the penis.
The chemical key to this entire process is nitric oxide (NO), released by the endothelial lining of the penile blood vessels. NO triggers the cascade of smooth muscle relaxation. Anything that reduces NO production or sensitivity, including smoking, vascular disease, and endothelial dysfunction, directly impairs erections at the source.
Timing matters for recovery. Reducing a specific cause, such as stopping smoking or addressing sleep deprivation, does not produce instant improvement. Endothelial health and hormonal balance recover over weeks to months, not days.
If chronic stress is part of the picture, strategies that modulate cortisol directly help. Research on ashwagandha, for example, has shown reductions in cortisol and improvements in testosterone in stressed men. The withanolides in ashwagandha article covers how this adaptogen works at the compound level.
What the Research Actually Shows
The 2025 PMC narrative review of ED in young men is the clearest synthesis of current evidence. It found that while psychogenic causes remain dominant in men under 40, a significant proportion also present with organic etiologies including endothelial dysfunction, hormonal imbalances, and metabolic syndrome. The assumption that young men with ED have “only” a psychological problem is clinically outdated.
A separate PMC review from Rastrelli and Maggi argued directly that young men with ED are often under-investigated, dismissed with reassurance rather than evaluated for the full spectrum of causes. This matters because missing an organic cause means missing a treatable condition.
The honest reality check: most young men with ED never see a doctor about it. They search online, try medication without a prescription, or suffer in silence. The gap between what research shows is possible in terms of recovery, and what men actually experience, is largely a gap in help-seeking, not in available solutions.
“ED in younger men is likely to be overlooked and dismissed without performing any medical assessment, even the most basic ones.” — Rastrelli & Maggi, Translational Andrology and Urology, PMC5313296
Side Effects and What to Watch Out For
Two things deserve honest mention here that usually get buried.
First: ED in a young man can be an early warning sign of cardiovascular disease. Penile arteries are smaller than coronary arteries. Endothelial dysfunction that is not yet causing chest pain or breathlessness may already be affecting erectile function. This is not a reason to panic. It is a reason to investigate rather than ignore.
Second: self-medicating with ED drugs like sildenafil (Viagra) without a diagnosis masks the problem without addressing it. These medications work by amplifying the nitric oxide signal, but they do not fix the underlying cause. If the cause is psychological, taking sildenafil without addressing the anxiety often creates dependence on the drug rather than resolution of the problem.
If you are also dealing with fatigue, mood changes, or poor recovery from exercise, hormonal causes are worth investigating. Our article on 7 signs of magnesium deficiency covers a mineral that affects both sleep quality and testosterone production, both of which are relevant here.
For those who smoke and are looking for leverage to quit: ED is one of the most reversible consequences of smoking when it is caught early. Endothelial function begins recovering within weeks of quitting.
Who Should Actually Do What?
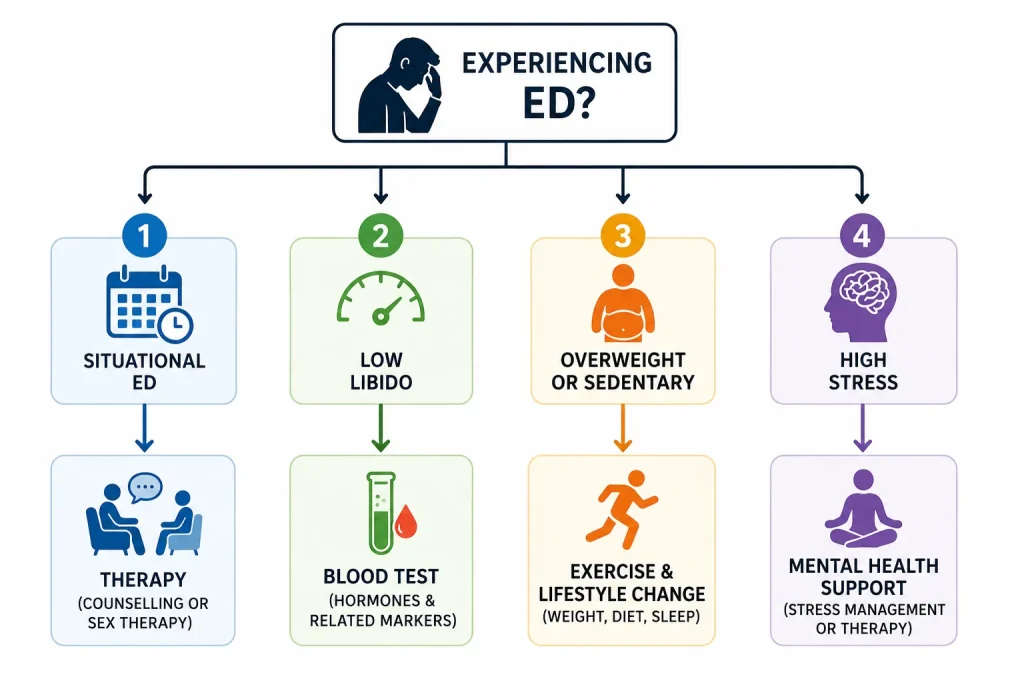
If Your ED Is Situational (Works Sometimes, Not Others)
Situational ED, where erections work during sleep, masturbation, or certain situations but fail with a partner or under pressure, is almost always primarily psychological. The body is physically capable. The obstacle is anxiety, stress, or arousal pattern.
Start here: reduce pornography use for 4 to 6 weeks, work on sleep quality, and consider speaking to a therapist trained in sex therapy or cognitive-behavioural therapy. These are not soft suggestions. They are the evidence-based first-line treatments.
If Your ED Is Consistent and Getting Worse
Consistent, progressive ED in a young man warrants a basic workup: fasting blood sugar, lipid panel, testosterone, thyroid function, and blood pressure. This is not overreacting. It is basic due diligence.
If organic causes are ruled out and psychological ones are present, a multidisciplinary approach combining medical support and psychological therapy produces better outcomes than either alone.
If You Are Overweight or Have a Sedentary Lifestyle
This category has the most modifiable risk. Visceral fat reduces testosterone through aromatase activity. Physical inactivity reduces cardiovascular fitness and nitric oxide production. Both are directly addressable.
Structured aerobic exercise, three to five sessions per week, has consistently shown improvements in erectile function in research populations, independent of other interventions. Start with walking, then build. Our article on how to lose fat by walking is a practical starting point.
On the dietary side, heart health and erectile health share the same nutritional foundations. The 10 best fruits for heart health article is directly relevant, since endothelial function responds to antioxidant-rich foods.
If You Are Under Severe Stress or Dealing with Depression
ED is a downstream symptom here, not the root problem. Treating the ED without treating the depression or anxiety typically fails. Speak to a psychiatrist or psychologist first. Many antidepressants themselves can cause sexual side effects, so honest discussion with a doctor about sexual health as part of mental health treatment is essential.
If You Suspect Hormonal Issues
Get a blood test. Specifically: total testosterone, free testosterone, LH, FSH, prolactin, and thyroid function (TSH, T4). Without these numbers, you are guessing. If low testosterone is confirmed, treatment options range from lifestyle interventions to medical management, but the decision requires a doctor.
The Bottom Line
Erectile dysfunction in young men is rarely about one single cause. It is usually a combination of psychological pressure, lifestyle habits, and sometimes underlying metabolic or hormonal issues that compound each other.
The most important thing to understand is this: ED in a young, otherwise healthy man is almost always reversible. But reversible does not mean it resolves on its own. It means the causes can be identified and addressed.
Do not self-diagnose and do not self-medicate. Get a basic workup, be honest about lifestyle and pornography habits, and take sleep and stress as seriously as any physical symptom. Those three steps cover the vast majority of cases.
The conversation is harder to start than the problem is to fix.
People Also Ask
Can stress alone cause erectile dysfunction in young men?
Yes. Stress activates the sympathetic nervous system, which releases adrenaline and constricts blood vessels throughout the body, including penile arteries. This physiological response directly prevents the blood flow needed for an erection. Chronic stress also raises cortisol, which suppresses testosterone production. In many young men, psychological stress is the sole or primary cause of ED, and addressing the stress resolves the erectile difficulty without any other intervention.
Is erectile dysfunction in your 20s permanent?
No. ED in young men is highly reversible in the majority of cases, particularly when the cause is psychological, lifestyle-related, or hormonal. Identifying the specific cause is the first step. Psychological ED typically responds well to therapy and anxiety management. Lifestyle-driven ED, including cases linked to obesity, smoking, poor sleep, or inactivity, responds to the corresponding lifestyle change. Even some organic causes, such as early endothelial dysfunction, show meaningful improvement with cardiovascular exercise and dietary change.
Does watching too much porn actually cause erectile dysfunction?
The evidence suggests it can, for some men, through altered arousal patterns rather than any physical mechanism. The clearest sign is situational ED: erections function normally with pornography but are absent or reduced with a partner. This pattern points to a dopamine reward system issue, not a physical one. There is no formal diagnosis for “porn-induced ED” in current medical classifications, but the psychological mechanism is scientifically plausible and frequently reported. Reducing or eliminating pornography use for several weeks is a reasonable, low-risk intervention to test whether it is a contributing factor.
What is a common sign of erectile dysfunction that young Indian men ignore?
Inconsistent erection quality during partnered sex while maintaining normal erections in the morning or during masturbation is the most commonly dismissed early sign. Many young men attribute this to tiredness or “just a bad night” and do not investigate further. This pattern, known as situational ED, is clinically meaningful and warrants attention rather than dismissal. In India, the reluctance to discuss sexual health with a doctor means these early signals often go unaddressed for years, allowing underlying causes to deepen.
Can low testosterone cause erectile dysfunction in young men?
Yes, though it is not the most common cause of ED in young men, it is increasingly prevalent. Low testosterone reduces libido, impairs the strength of arousal signals, and affects the health of erectile tissue. The causes of low testosterone in young men are largely lifestyle-driven: obesity, chronic sleep deprivation, high stress, and poor diet all suppress testosterone production. A blood test is required to confirm. Many men experiencing both ED and symptoms like low energy, reduced motivation, and poor gym performance may have an underlying hormonal component worth investigating.
Is erectile dysfunction always a sign of heart disease?
Not always, but it can be an early warning sign in some cases. Penile arteries are among the smaller blood vessels in the body and can show signs of endothelial dysfunction before larger coronary arteries do. Research has found that young men with ED have, on average, higher blood pressure, cholesterol, and inflammatory markers than age-matched controls. This does not mean everyone with ED has heart disease. It means that progressive or unexplained ED in a young man warrants basic cardiovascular screening, not just reassurance.
Can diet affect erectile function in young men?
Yes, significantly. A diet high in processed foods, refined carbohydrates, and low in vegetables, healthy fats, and micronutrients contributes to endothelial dysfunction, elevated blood sugar, and reduced testosterone, all of which impair erectile function. A diet rich in antioxidants, nitrate-containing vegetables like leafy greens and beets, and adequate zinc and magnesium supports vascular and hormonal health. This is not a miracle cure, but the nutritional foundations of cardiovascular health and erectile health are the same.